
Birth
Watching labor unfold can feel overwhelming. Learn how breath supports each stage of labor and

What if every person in labor had someone by their side whose only job was

Discover 4 evidence-based pain coping tools for labor. Time-tested strategies from a doula and prenatal

To support alignment, ease common pregnancy discomforts, and help students feel strong and comfortable throughout

One of the most common concerns I hear from expectant parents is, “What if my
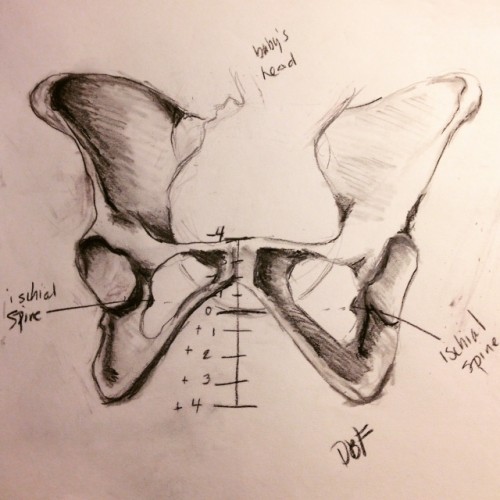
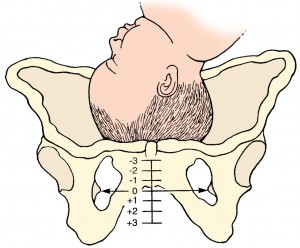
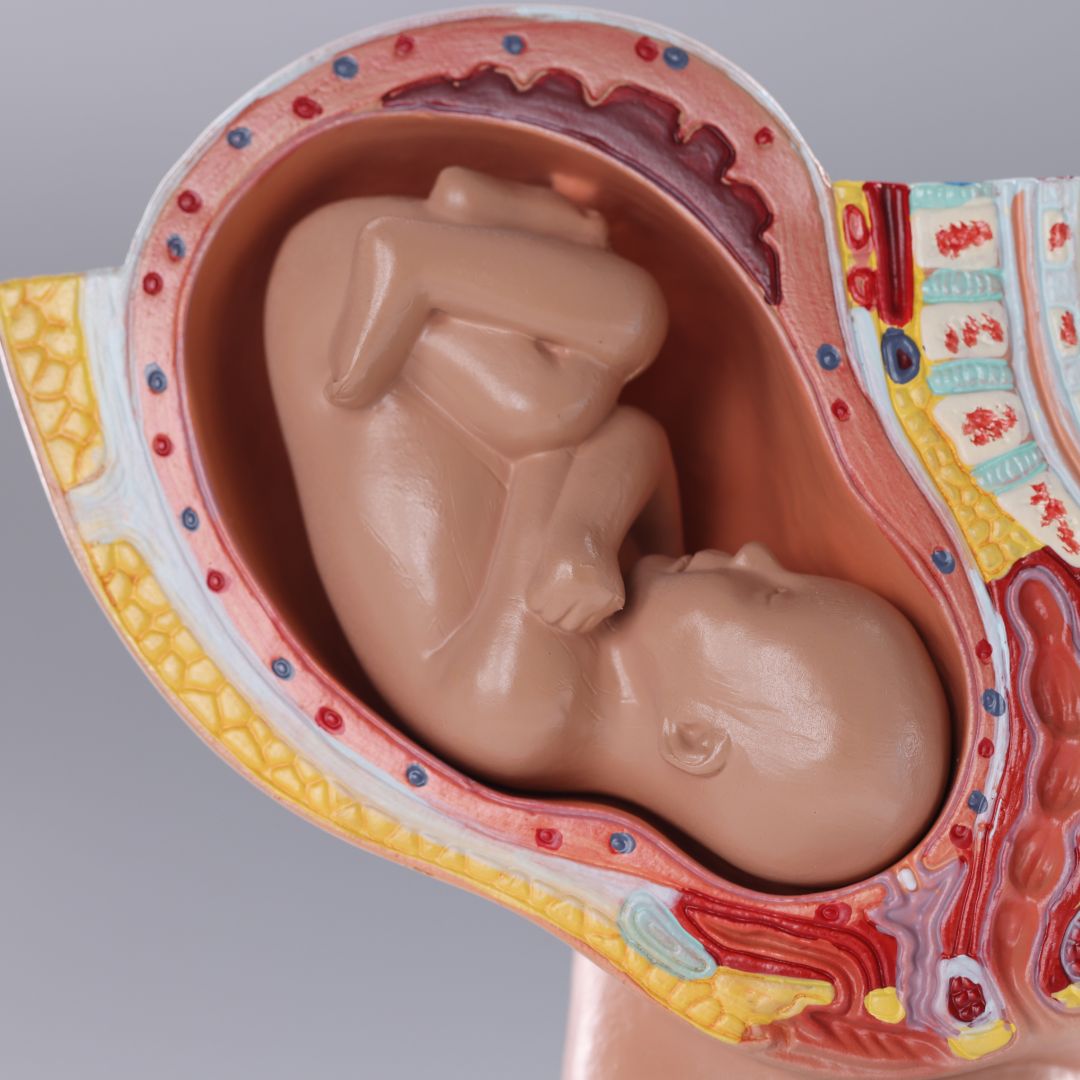
It’s not just about dilation—station matters too! Station refers to how low the baby is

When we experience pain—whether it’s from an injury, illness, or labor—our instinct is often to

Prenatal yoga is a wonderful way to strengthen, create mobility and learn coping skills needed

Navigating the opinionated landscape of breastfeeding can be a daunting task. It’s easy to feel
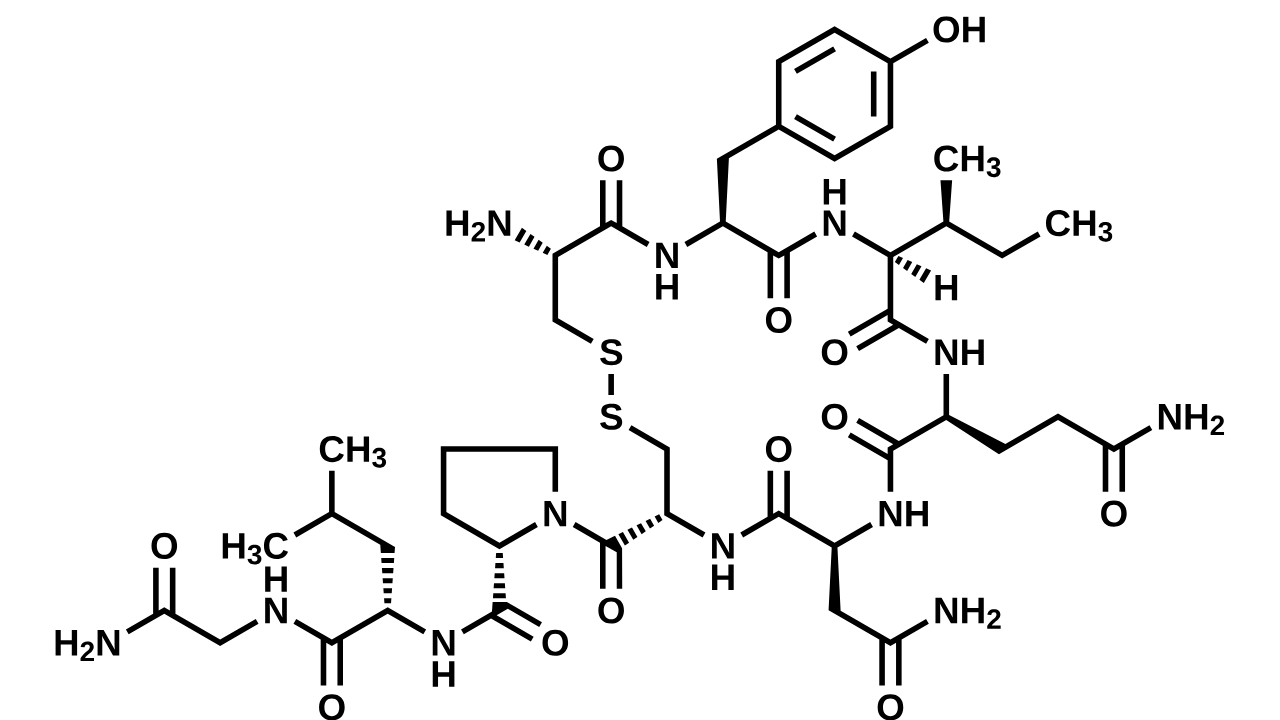
Learn about oxytocin, beta-endorphins and adrenaline, the hormones of labor, and how they may impact
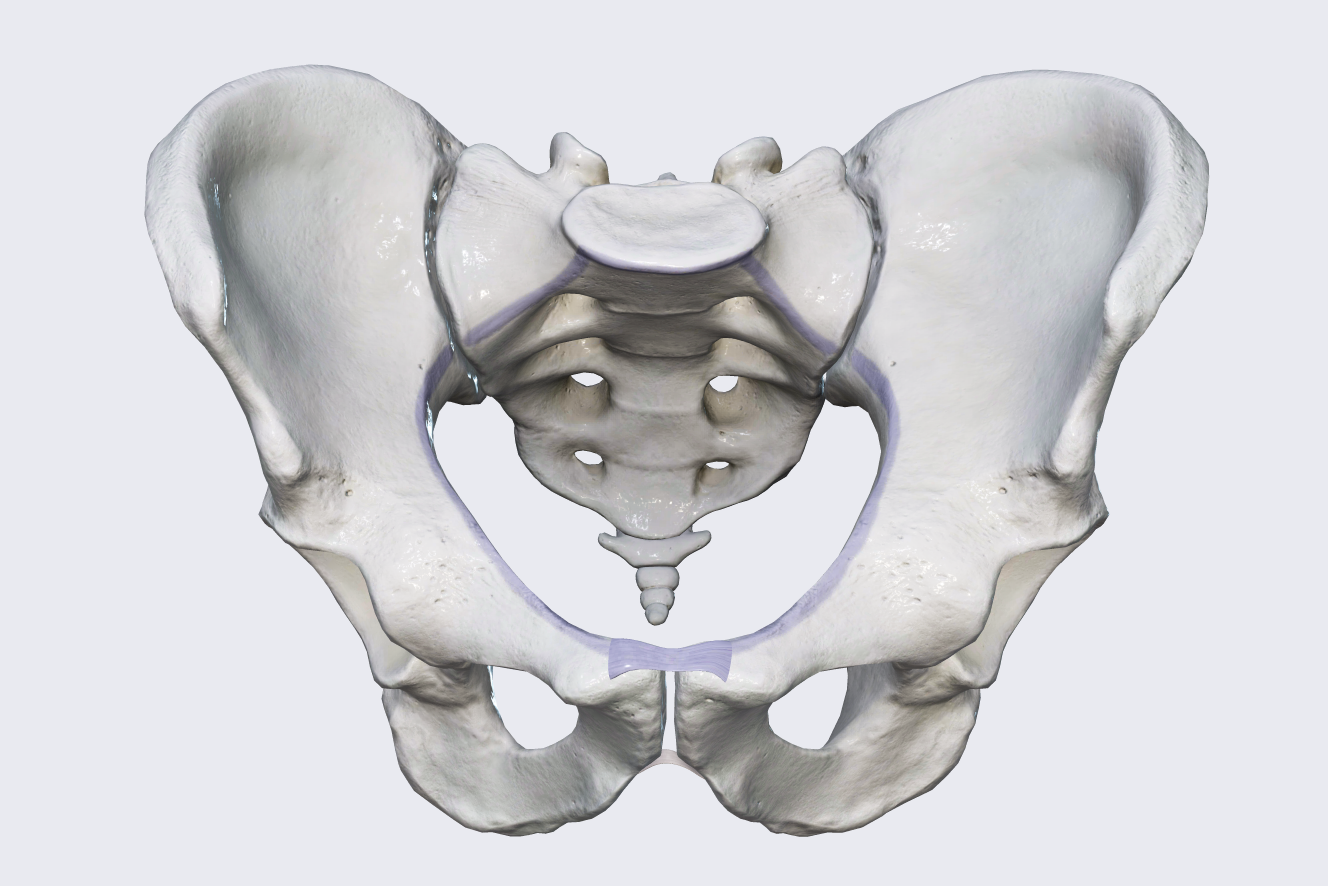
The Pelvis is not a fixed entity. There are joints which allow for the pelvis
If you’re considering an elective induction or facing a medical induction, it may be helpful

Not long ago, a student returned to postnatal yoga after giving birth to her first

The World Health Organization estimates that around 13% of people worldwide who have recently given

Prenatal Yoga – A Natural Path toward Working with a Midwife by Risa Klein, CNM,

Diastasis recti (separation of the rectus abdominis) affects all expectant folks to some degree. However,

Learn how breastfeeding may be impacted by epidurals and how to alleviate the difficulties they

Learn how to safely modify your prenatal yoga practice and which yoga poses to avoid

Discover these easy prenatal yoga modifications and try adding them to your regular yoga practice.

Discover effective ways for your partner to support you during pregnancy and labor and explore

A few weeks ago, one of my good friends was facing labor induction. She was

Discover the role the psoas muscle plays in pregnancy, birth and postpartum recovery and how
Discover why umbilical knots and nuchal cords aren’t as concerning you may think and learn

Learn about what a postpartum doula does and why hiring one can help you to

Discover seven prenatal yoga poses that can help to prepare your pelvis for birth by


